
The concept of ventilation was first introduced when man brought fire into the home and discovered the need to let smoke out and supply air to keep the fire burning. It wasn’t until the mid to late 1800s that the first estimate of a minimum ventilation rate was published based on calculations of the amount of fresh air needed to purge CO2 from the lungs. This estimate was based off of metabolic needs but proved to be too little ventilation for comfort’s sake (Janssen 1999). Subsequent efforts to estimate an acceptable minimum ventilation birthed a contradiction in ventilation design that still rings true to this day: should ventilation be based on physiological needs, on comfort, or on health?
The most authoritative American work on minimum ventilation estimates came from a physician named J. Billings in the late 1800s. He argued for higher ventilation rates because he was concerned about the spread of disease, particularly tuberculosis. In 1895, ASHVE (American Society of Ventilation Engineers) “adopted the view that engineers were ready to accept the ideas of hygienists and physiologists” (Klauss et al. 1970). They recommended 30 cfm (14 L/s) per person as a minimum and placed responsibility of design and construction on engineers.
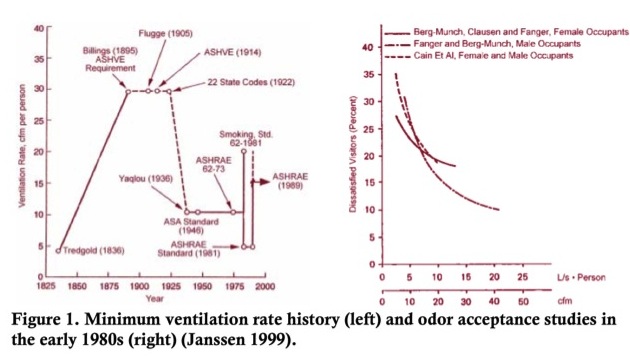
For centuries a ventilation dichotomy existed between engineers and physicians. Engineers were concerned with providing comfort and reducing odors and CO2 accumulation while physicians were concerned with minimizing spread of disease. After much research on comfort, odors, and recirculation throughout the early 1900s, ASHVE (now ASHRAE - American Society of Heating, Refrigerating, and Air Conditioning Engineers) published a guide in 1925 setting the minimum ventilation rate to 10 cfm (4.7 L/s) per person. This remained until the 1980s, when multiple studies found that 15 cfm (7.5 L/s) of outdoor air was sufficient to reduce concentrations of tobacco smoke to an odor level acceptable by 80% of the population (graph on the right in Figure 1). The graph on the left in Figure 1 shows the history of minimum ventilation rates in the United States, peaking right after the Civil War when disease transmission was the primary cause of death. Minimum ventilation rates were reduced again after many research efforts on odor and comfort as well as advances in HVAC technology. The current ASHRAE Standard 62 determines the minimum outdoor air intake rates from various parameters such as space type, space application, occupancy level, and floor area. Intake rates are also highly dependent on outdoor air quality.
 An extensive literature review published in 2011 judged 27 papers that provided sufficient information on both ventilation rates and health effects to inform the relationship (Sundell et al. 2011). Higher ventilation rates of 25 L/s per person (~53 cfm/person) were associated with reduced prevalence of sick building syndrome symptoms, and inflammation, respiratory infections, asthma symptoms, and short-term sick leave increased with lower ventilations rates. The authors note that while the articles they identified support a positive benefit with ventilation rates above the current ASHRAE standards, the need remains for more studies of the relationship between ventilation rates and health (specifically those that tackle the difficult methodological challenges of measuring ventilation properly).
An extensive literature review published in 2011 judged 27 papers that provided sufficient information on both ventilation rates and health effects to inform the relationship (Sundell et al. 2011). Higher ventilation rates of 25 L/s per person (~53 cfm/person) were associated with reduced prevalence of sick building syndrome symptoms, and inflammation, respiratory infections, asthma symptoms, and short-term sick leave increased with lower ventilations rates. The authors note that while the articles they identified support a positive benefit with ventilation rates above the current ASHRAE standards, the need remains for more studies of the relationship between ventilation rates and health (specifically those that tackle the difficult methodological challenges of measuring ventilation properly).
Historically the argument for a better indoor environment, whether it was a solution for odors (Figure 1) or disease transmission, was to increase the amount of outdoor air supplied to the space. We have now reached a point where a third factor is heavily influencing standards for mechanical ventilation: energy usage. With increasing concerns regarding depletion of fossil fuels, global climate change, and CO2 emissions, it is important to note that 41% of U.S. energy consumption can be attributed to buildings (DOE 2011). Particularly, approximately 50% of a building’s total energy consumption is used to operate the heating, ventilation, and air conditioning (HVAC) systems of that building (EIA 2003). There is now an increasing push for more energy efficient, tight, and “green” buildings. The number of LEED (Leadership in Energy and Environmental Design) Certified buildings has been steadily increasing over the past 10 years. LEED is a green building certification program run by the U.S. Green Building Council (USGBC). LEED concentrates its efforts on improving building performance across five key areas of environmental and human health: energy efficiency, indoor environmental quality, materials selection, sustainable site development, and water savings. The USGBC describes its LEED program as “a nationally accepted benchmark for the design, construction and operation of high-performance green buildings” and “provides building owners and operators with the tools they need to have an immediate and measurable impact on their buildings’ performance.”
In January of this year, mayors from ten major American cities announced that they will participate in a united effort (called the City Energy Project) to significantly boost energy efficiency in their buildings (NRDC 2014). Engineers designing and maintaining building ventilation systems are encountering a new ventilation dichotomy: How do we move towards more energy efficient buildings without compromising indoor air quality and its subsequent health effects? Providing the minimum required ventilation results in less energy use by the HVAC system, but is this standard sufficient to reduce risk of disease transmission and promote a healthy and productive space? Are there more effective or energy efficient options for promoting a healthy and productive environment besides increasing the amount of outdoor air supplied? Or are there other options that can be used in a building to decrease the energy use while maintaining adequate ventilation for health?
References:
Janssen, J.E., 1999. The History of Ventilation and Temperature Control. ASHRAE Journal, 41, pp.47–52.
Klauss, A.K. et al., 1970. History of Changing Concepts of Ventilation Requirements. ASHRAE Journal, 12(6).
Sundell, J. et al., 2011. Ventilation rates and health: multidisciplinary review of the scientific literature. Indoor Air, 21(3), pp.191–204. Available at: http://www.ncbi.nlm.nih.gov/pubmed/21204989 [Accessed March 28, 2013].
DOE, 2011. Buildings Energy Data Book, Available at: http://buildingsdatabook.eren.doe.gov/ [Accessed October 2, 2010].
EIA, 2003. Commercial Buildings Energy Consumption Survey (CBECS) Data, Available at: http://www.eia.gov/consumption/commercial/data/2003/ [Accessed February 18, 2014].
NRDC, 2014. Ten large US cities join major new initiative to reduce carbon pollution from buildings | Kaid Benfield’s Blog | Switchboard, from NRDC. National Resources Defence Council Press Release. Available at: http://switchboard.nrdc.org/blogs/kbenfield/ten_large_us_cities_join_major.html?utm_source=tw&utm_medium=tweet&utm_campaign=socialmedia [Accessed March 29, 2014].
